Introduction
Oral health refers to the conditions of an individual’s mouth including; the teeth, gums and other related oral tissues. Oral health affects people physically and psychologically; and influences how they thrive, look, speak, eat and socialise; as well as contributing to feelings of social wellbeing (1).
Oral health is an important Public Health issue, due to its association between oral diseases and deprivation, as well as being largely preventable. It has implications in the form of tooth decay, tooth erosion, gum disease, oral cancer and even systemic health issues like cardiovascular disease and diabetes complications (1).
Tooth decay has a lifelong impact as poor childhood dental health is a predictor of poor adult dental health. Whilst oral has improved over the last few decades dental decay is still a leading cause of childhood hospitalisation with an estimated cost of £14.5 million in 2014/15 (2). The COVID-19 pandemic has also significantly impacted oral health and oral health inequalities, which have been further compounded by the cost of living crisis (3).
The purpose of this topic overview is to provide a summary of some of the key indicators, relating to oral health in adults and children, to raise awareness and highlight preventative initiatives, which could help alleviate the burden it presents.
Risk factors
Oral diseases are socially patterned and disproportionately affect people living in more deprived and marginalised communities. Oral Health and General Health and inextricably linked as they share common risk factors
The modifiable risk factors for oral disease include: having a diet high in sugar, smoking or chewing tobacco, alcohol, poor oral hygiene and irregular use of dental care services (1).
Certain communities are more likely to have poor oral health and are less likely to use dental services. These include children, the elderly, individuals with learning disabilities deprived populations and those in institutional care (1).
Issues such as not being able to afford basic dental health items such as a toothbrush or toothpaste or not being able to afford travel to dentists have also been highlighted as a compounding issues.
Access to Dental Services
NHS dentistry provides treatment that is clinically necessary and includes primary, community, urgent out of house dental services, secondary and tertiary dental services (3). There are patient charges in place for NHS dentistry with only specific groups exempt and entitled to free NHS Dental treatment in England (3).
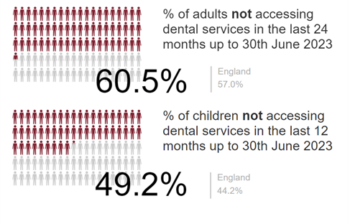
Figure 1 shows the % of adults in the NHS Devon ICB not accessing dental services in the last 24 months (District not available). Almost 2 in 3 adults and 1 in 2 children are not accessing dental services (4).
Figure 1: Data for NHS Devon Integrated Care Board
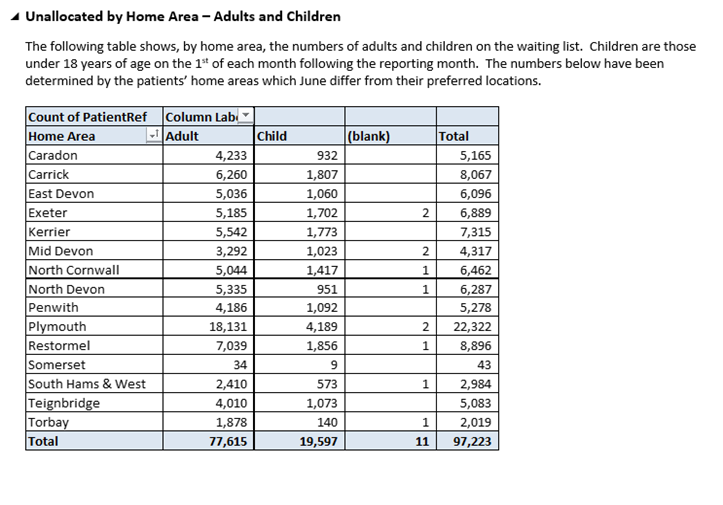
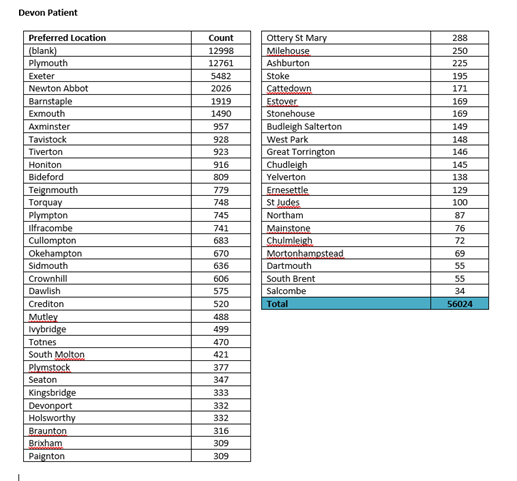
Adults and children in Exeter, East Devon and Teignbridge have the highest waiting list figures by home area. Please note that Torridge figures are not available (see Appendix i home area June 2024*). At ward level Exeter, Newton Abbot and Barnstaple are highest for those waiting for a dentist in their preferred area (see Appendix ii preferred area April 2024*).
Adults and children accessing dental services is still seeing some of the impact from the pandemic (5). There also appears to be district variations, which could be attributed to levels of deprivation (5).
Child Oral Health Indicators
18.1% of 5-year-old children in Devon have experience of dental decay. Compared with 23.7% in England. The lowest % presentation of dental decay was in South Hams at 8.3% and the highest in North Devon at 22.4% (6).
In relation to tooth extractions in hospital for 0-19 years olds, there is evidence of a higher prevalence in Devon when compared to national figures. Devon has a rate of 272.0 per 100,000 for tooth extraction, with tooth decay as primary diagnosis. This compares to 236.0 for England. The lowest rate is in Exeter at 98.7 and the highest is 580.2 in North Devon (7).
Adult Oral Health Indicators
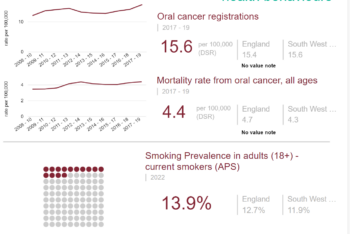
Current data around adult oral health is limited. Figure 3 shows figures for oral cancer registration and mortality for Devon appear to be in line with England figures. Smoking prevalence is slightly higher than England at 1.2% (4).
Figure 2: Data for the Devon County as a whole