Contents
1. Introduction
The last two annual reports have focused on COVID-19, examining how the pandemic has impacted families and communities and how the pandemic, along with the cost-of-living crisis, has exacerbated health inequalities, hitting the most vulnerable members of society hardest. The pandemic has resulted in a significant rise in demand for health and care services and excess mortality. The demand has been driven by a combination of lifestyle factors, people delaying seeking medical help and disruption to the health and care system. We also know demand for health and care services is linked to the conditions in which we are born into, grow, live, work and age, known as the wider determinants of health. This year’s annual report focuses on prevention and why now more than ever, it is vital that we invest in prevention.
While there can be no doubt the pandemic has had a negative impact on the public’s health, the reality is that the health of the population has not been improving for the past decade. Sir Michael Marmot was commissioned by the British Government to review health inequalities in England in 2010 (Fair Society, Healthier Lives) and following publication of this report was asked to undertake a 10-year review which he published in 2020 just before the pandemic. The report entitled ‘Health Equity in England: The Marmot Review 10 years on’ (Health Equity in England) presented a stark picture. He discovered that life expectancy has stalled for the first time in 100 years and in some cases, such as women in the most deprived communities, has fallen and health inequalities have widened. Worse still, not only has life expectancy stalled but the amount of time people are spending in good health, measured as healthy life expectancy, has reduced. The people living in the most deprived communities are getting old before their time, living shorter lives and spending more of their short lives in poor health.
Much of this poor health and premature death is largely a result of preventable diseases. The global burden of disease shows that cancer followed by cardiovascular disease (CVD), and then respiratory disease are the leading cause of death in adults and make the largest contribution to years of life lost and therefore have the biggest impact on life expectancy (Understanding the drivers of healthy life expectancy: report ) Modifiable risk factors such as tobacco, diet, alcohol and physical inactivity contribute greatly to these diseases. Tobacco is the risk factor making the largest contribution to years of life lost for both sexes, followed by Obesity, high cholesterol and high blood pressure (Understanding the drivers of healthy life expectancy: report )
We also know that modifiable risks factors are more prominent in the most deprived communities, and it is this that drives inequalities in health outcomes. While preventative programmes need to be available to all, to tackle inequalities it is critical that focus should be given to those in greatest need. Targeted behavioural change programmes, screening and immunisation programmes at those in greatest need is critical.
The financial case for investing in some preventative programme is very strong (Cost effectiveness of public health programmes). The overall cost effectiveness and return on investment both in the short-term and longer-term is evident for some preventative programmes. Programmes optimising detection and management of people at an increased risk (QRISK of 10% or more) of developing a heart attack or stroke within the next 10 years, are well evidenced as having a short-term return on investment. But also programmes which focus on the detection and management of diabetes or falls prevention programmes demonstrate an excellent return on investment in the longer-term, reducing future costs on the health and care system. The evidence also points to respiratory disease and cardiovascular disease being a key driver of the current demand in A&E admissions and urgent care, so targeted programmes as described above, are not only an effective use of limited NHS resources, but they contribute to addressing health inequalities, and critically help tackle the increasing demand for health services (NHS England Board paper December 2022).
We also understand that circumstances impact on an individual’s ability to make healthier choices. Addressing modifiable risk factors as families struggle with the current economic crisis with local data suggesting food insecurity levels in Devon at 29% and 13% of households living in fuel poverty is a real challenge. It is therefore important that when we think about prevention, we recognition that the wider determinants of health impact greatly on individuals and families so tackling the root causes of the conditions in which the most vulnerable people in Devon find themselves is vital.
The South West has recently been designated a Marmot Region which will bring a renewed focus at a regional level on tackling health inequalities. Being a Marmot region will allow us to have access to experts in tackling health inequalities and learn from Marmot Regions and Marmot Cities from around the country. We will actively work with colleagues locally to ensure that the learning from being a Marmot Region is actioned locally.
The Devon Integrated Care Strategy, the 5-year Joint Forward Plan captures the key challenges facing Devon. The Plan includes the need to consider and tackle the wider determinants of health, housing and the economy for example but also the need to enhance prevention activity and tackle inequalities. The Plan provides a real opportunity for the health and care system to work more collaboratively on the key priorities for Devon to improve health outcomes for residents.
We have all heard the saying ‘prevention is better than cure’ and while everyone would agree with this statement, the reality is that central government funding for prevention has been reducing in real terms over recent years. Evidence-based preventative action targeted at the right communities, families and individuals is cost-effective not only in the longer-term but also in the short and medium term. It is now more important than ever to increase prevention investment and scale up evidence-based prevention programmes. Enhanced action now will help reduce the growing demand on the health and care system, contribute to the increasing financial challenges and most importantly increase healthy life expectancy for Devon residents and impact on health inequalities.
Steven Brown; Director of Public Health, Communities and Prosperity
Recommendations:
- Devon Integrated Care Partnership should work together to realise the potential they have as anchor institutions to improve the lives of local people and reduce health inequalities, drawing on evidence of the impact of this approach from other areas.
- Devon Health and Wellbeing Board to consider the impact of the climate emergency on health and equity, through the production of a joint strategic needs assessment; The board should review, adopt and monitor the partnership’s climate change mitigation and adaptation plans and the opportunities they present to create a fairer, healthier, more resilient and more prosperous society.
- Public Health Devon to actively work with system partners to support the delivery of the agreed Joint Forward Plan objectives and actions in relation to taking the wider determinants of health.
- Public Health Devon to actively participate in the Marmot Region work programme and ensure learning is shared with Integrated Care Partnership.
- The Devon Food Partnership and the Energy Saving Devon partnership utilise every opportunity to address health, equity and the climate emergency through their collective programmes.
- Public Health Devon and Devon Integrated Care Partnership to work collaboratively with communities within multi-agency alliances, to develop and refine multi-level programmes of action on the leading modifiable risk behaviours (tobacco, food, excess weight, alcohol, physical inactivity), ensuring there is an appropriate mix of individual and population level approaches to make an impact at pace and scale.
- Public Health Devon to work with stakeholders in Devon Integrated Care Partnership to develop and implement a programme of professional development to upskill the workforce in compassionate, health gains approaches to healthier weight to destigmatise individual behavioural change interventions, promoting confidence and emotional wellbeing.
- Public Health Devon to work with system partners to test place-based approaches to drive community-based prevention action. These should be designed with and informed by local communities, utilise community assets and act on clustered risks, utilising proxy measures to demonstrate impact in the short to medium term.
- Through the Population Health Management programme, the Devon Integrated Care System should implement a range of data-based approaches for case finding for avoidable conditions or to improve outcomes. These methods should focus on detecting the precursors and early stages of disease, design preventive interventions and monitor their impact.
- Following the success of the Devon mass vaccination inequalities cell through the Covid-19 pandemic, the application of a multi-disciplinary inequalities cell approach to secondary prevention programmes to drive action around community engagement and targeting and reducing inequalities.
- There should be equity in access to services and all levels of preventative support including screening and vaccination, with proactive community engagement and reasonable adjustments where needed building on learning from outreach work during the pandemic.
2. Scene Setting

Put simply prevention is the action of stopping something from happening. To define prevention in a public health text we need to understand the different contexts in which prevention occurs. Health and wellbeing is influenced by a range of social, economic and environmental factors known as wider determinants and action in their areas can improve health and wellbeing in the population and reduce the burden of disease. Direct public health action to prevent ill health is grouped into primary prevention, which involves specific action to stop illness developing in the first place; secondary prevention, which involves detecting the early stages of disease to take action before more severe harm has occurred; and tertiary prevention, which is softening the impact of existing illness to improve quality of life. These are defined in more detail in the diagram below. Action in the real world is complex and rarely fits neatly with definitions, with work in public health often crossing over between these different areas. Whilst the chapters of this report describe work on the wider determinants, and primary, secondary and tertiary prevention, it is important to understand that these approaches are complimentary and do often overlap.
Figure 2.1 What is Prevention?
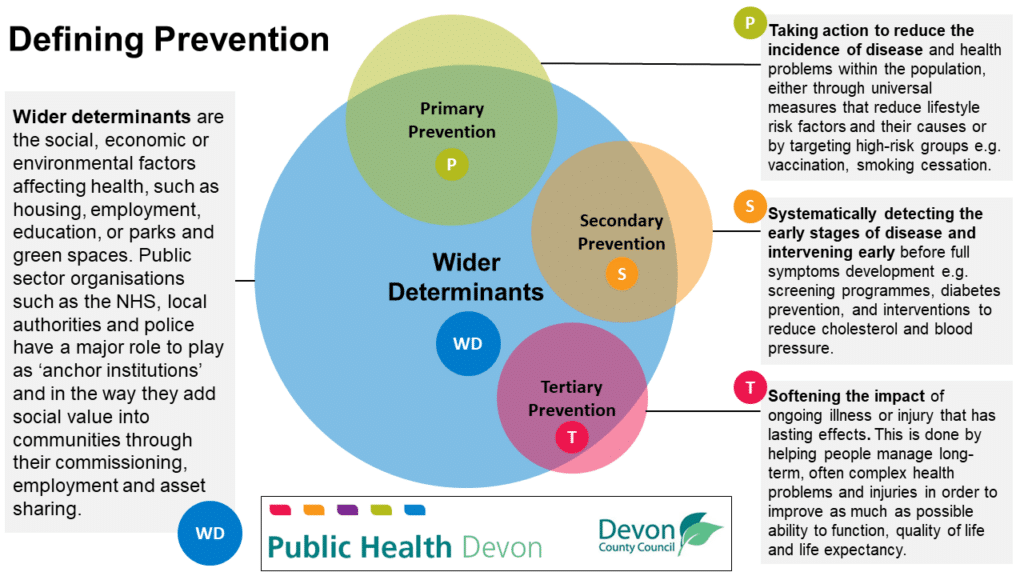
Adapted from Local Government Association: Prevention Definition and Duties and One Gloucestershire
To understand the context and the need for prevention, we also need to understand the current health and wellbeing challenges facing our society.
The increases in life expectancy seen throughout the modern era have stalled over the last decade (figure 2.2). The reasons for this are many and complex, including:
- Economic: 2008 Credit Crunch and subsequent economic downturn, the impact of Covid-19 lockdowns and the current cost-of-living crisis from 2020 onwards
- Changing disease patterns: the emergence of Covid-19 and changing patterns of infectious diseases (including healthcare associated and anti-microbial resistance), increasing ‘deaths of despair’ associated with substance misuse and suicide, and increases in deaths and ill health relating to risk factors such as excess weight
- Cohort effects: pre-2010 improvements due to health of ‘golden generation’ born in early 1900s who benefitted most from post-war stability and economic development
- Climate emergency (heat, pollution, ecosystem): Already impacting health with 5.5% of mortality in England and 4.6% of mortality in Devon attributable to air pollution (Public Health Outcomes Framework – Data – OHID (phe.org.uk)), and likely to increase in years to come.
Figure 2.2, UK Average Life Expectancy, 1901 to 2020
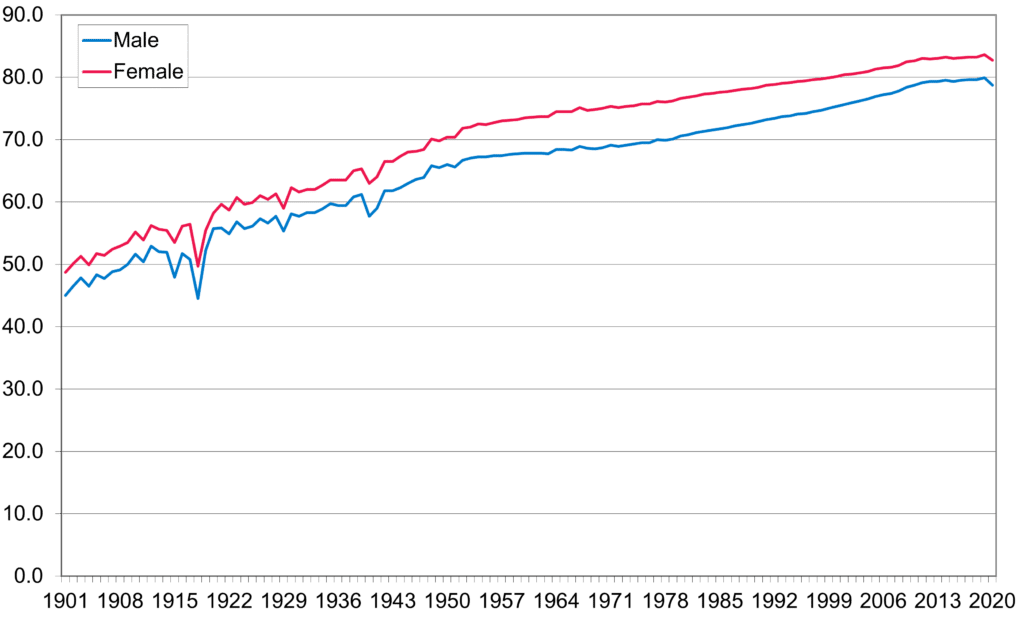
Source: Office for National Statistics, 2022
As well as the improvements in life expectancy stalling, levels of ill health and disability have increased. Figure 2.3 highlights an increase in the proportion of the working-age population who are long-term sick, increasing from around one in seven people in 2013 to around one in six in 2021. This equates to over 1.8 million adults in the UK who are unable to work because of long-term sickness, of which the majority are aged 50 and over. The number has increased 10% or 172,000 in three years.
Figure 2.3, Proportion of UK working-age population who are long-term sick, 2004 to 2022
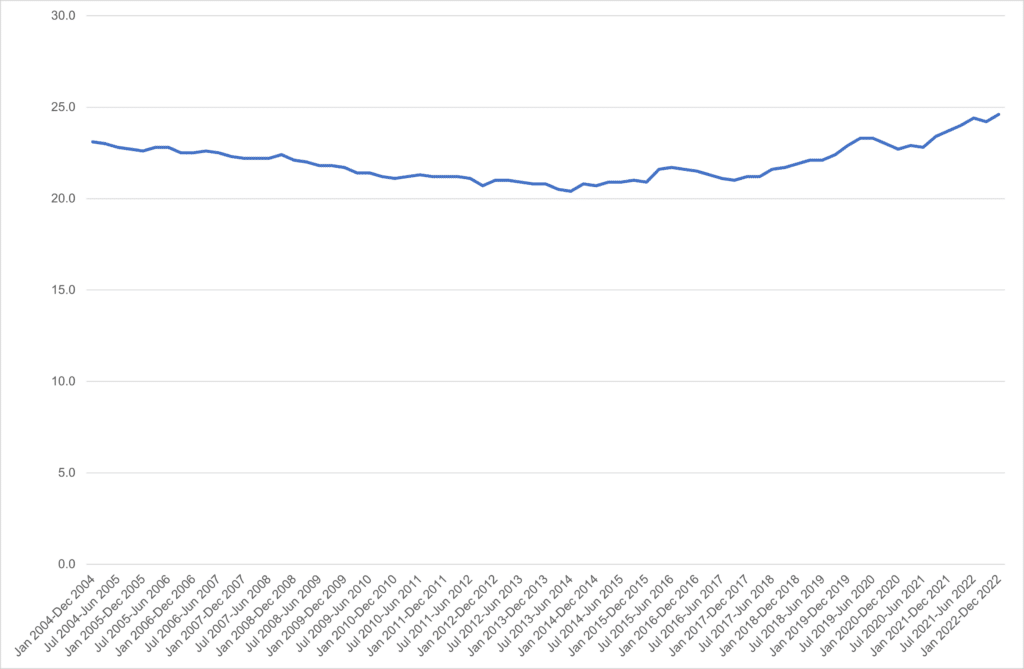
Source: ONS Labour Force Survey, www.nomisweb.co.uk, 2022
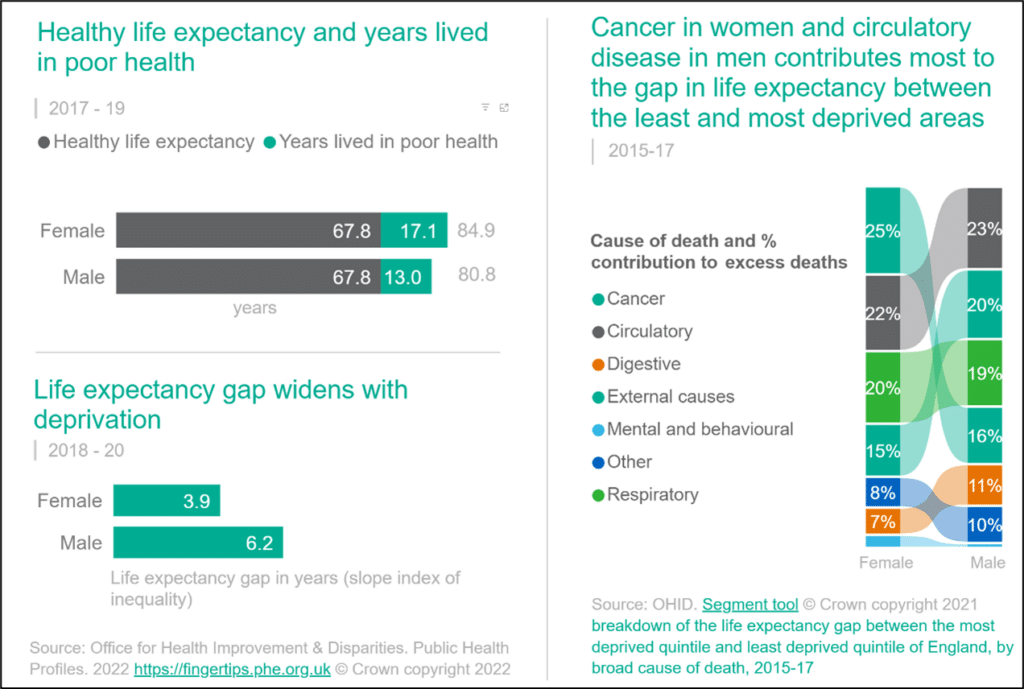
The impact of increased ill health and disability in the population is not felt equally. Figure 2.4 compares deprivation (horizontal axis) with average life expectancy and healthy life expectancy by Devon neighbourhood (MSOA), for males and females. More deprived communities experience much shorter healthy life expectancy and total life expectancy. A larger gap for healthy life expectancy means people in poorer communities spend more years of their life in poor health as well as dying younger. The gap between average healthy life expectancy between males and females is also narrower than overall life expectancy, also mean females typically spend more years in poorer health.
Figure 2.4, Life Expectancy and Healthy Life Expectancy by Deprivation, Devon Middle Super Output Areas, 2009-13
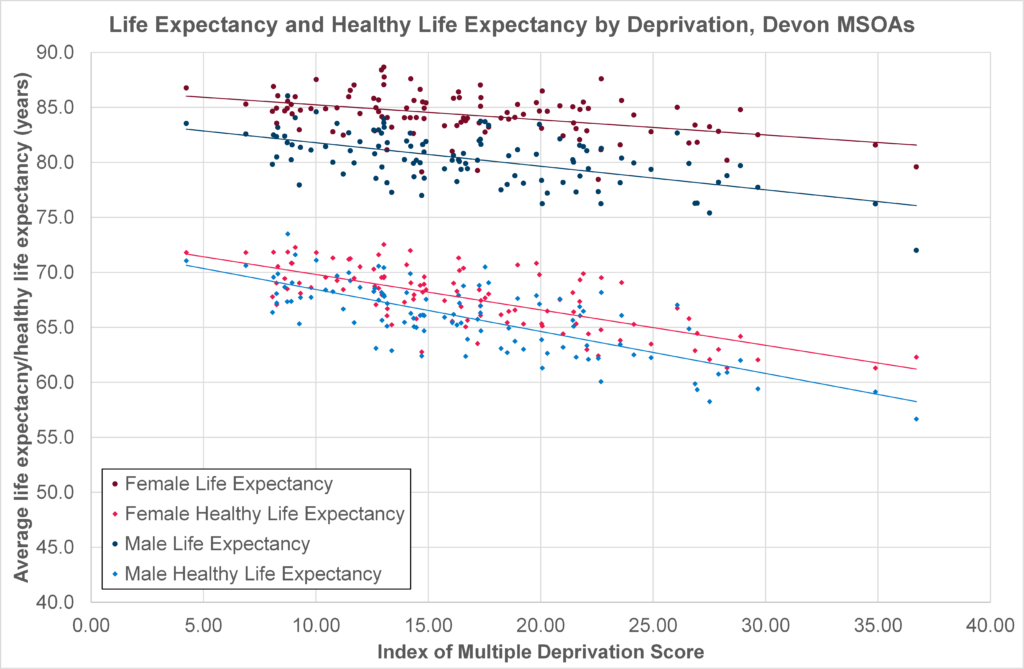
Source: Office for National Statistics
The health inequalities gap in life expectancy is also highlighted within the slope index of inequality (SII) measure, which compares expected life expectancy for different areas in relation to the deprivation profile. Figure 2.5 reveals an average SII gap of 6.2 years between the most and least deprived areas of Devon for male life expectancy, and 3.9 years for female life expectancy. The figure also highlights the conditions contributing most to the gap, with circulatory disease (contributing to 22% of the gap for females and 23% of the gap for males), cancer (25% for females, 16% for males), respiratory conditions (20% for females, 19% for males), and external causes such as accidents and self-harm (15% for females, 20% for males) respectively accounting for the greatest inequalities.
Figure 2.5, Life Expectancy Gap and Causes in Devon, 2015-17
Source: A Picture of Health, Office for Health Improvement and Disparities, 2023 Microsoft Power BI
In addition to the human impact of ill health, disability and premature death there is a financial one. The NHS ‘All Our Health’ strategy (Health disparities and health inequalities: applying All Our Health – GOV.UK (www.gov.uk) highlighted that prior to the Covid-19 pandemic health inequalities were estimated to cost the NHS an extra £4.8 billion, society around £31 billion in lost productivity and between £20 and £32 billion in lost tax revenue and benefit payments, with the challenges of the last few years likely to have increased these impacts further. On a Devon scale, these costs would run into tens of millions for NHS expenditure and hundreds of millions for wider societal impacts.
Pressures on health and care services in recent years, driven by population change, health inequalities and the economic impacts of the Credit Crunch, Covid-19 pandemic and cost-of-living crisis has also marked with reductions in levels of funding for preventive and early intervention services. A recent independent review of the integrated care system (Hewitt Review 2023) recommended the NHS spend on prevention should be increased by at least 1% over the next 5 years if we wish to improve population health and reduce pressure on the health and care system. The Government has recently published its response to the Hewitt Review (Governments response to the Hewitt Review). The response re-emphasised its commitment to tackling health disparities to enable people to live healthy lives and pointed to the yet to be published major conditions strategy which will outline how we need to shift the health system model towards preserving good health and early detection and treatment of diseases.
There is a clear and urgent case for a stronger focus on prevention. Whilst there is a time lag for the impact of some preventive interventions, this should not deter action. Interventions with individuals with established disease or conditions such as cardiovascular disease and diabetes can have an immediate or short-term impact (0-5 years); interventions through lifestyle and behavioural change can have a short-term and medium-term impact such as stopping smoking and alcohol misuse (0-5 years and 5-10 years) and interventions to modify the social determinants such as strengthening primary care, employment and housing will have a long-term impact. (10-15 years). Need to strengthen this section to make the economic case for investing in prevention.
3. The building blocks of health: the wider determinants

To protect and promote the health and wellbeing of Devon’s residents the right building blocks need to be in place: stable jobs, good pay, quality housing and good education for people of all ages. The difference in health outcomes for people in Devon arise from a complex interaction of many factors – housing, income, education, social isolation, disability – all of which are strongly affected by economic and social status.
To improve health for all of us and to reduce these unfair and unjust, and largely preventable inequalities in health, action is needed. Marmot’s ‘Fair society, healthy lives’ (2010) The Marmot Review outlined an evidenced based strategy to reduce these inequities. He describes how:
‘Action on health inequalities requires action across all the social determinants of health, including education, occupation, income, home and community. Not only is there a strong social justice case for addressing health inequalities, there is also a pressing economic case. It is estimated that the annual cost of health inequalities is between £36 billion to £40 billion through lost taxes, welfare payments and costs to the NHS.’
Dame Carol Black’s review (Black Review) also highlighted the huge economic costs of failing to act on the wider determinants of health. The key building blocks that affect our health and wellbeing – the wider determinants of health – are described by this diagram and represented in the outer layers.
Figure 3.1, The Wider Determinants of Health
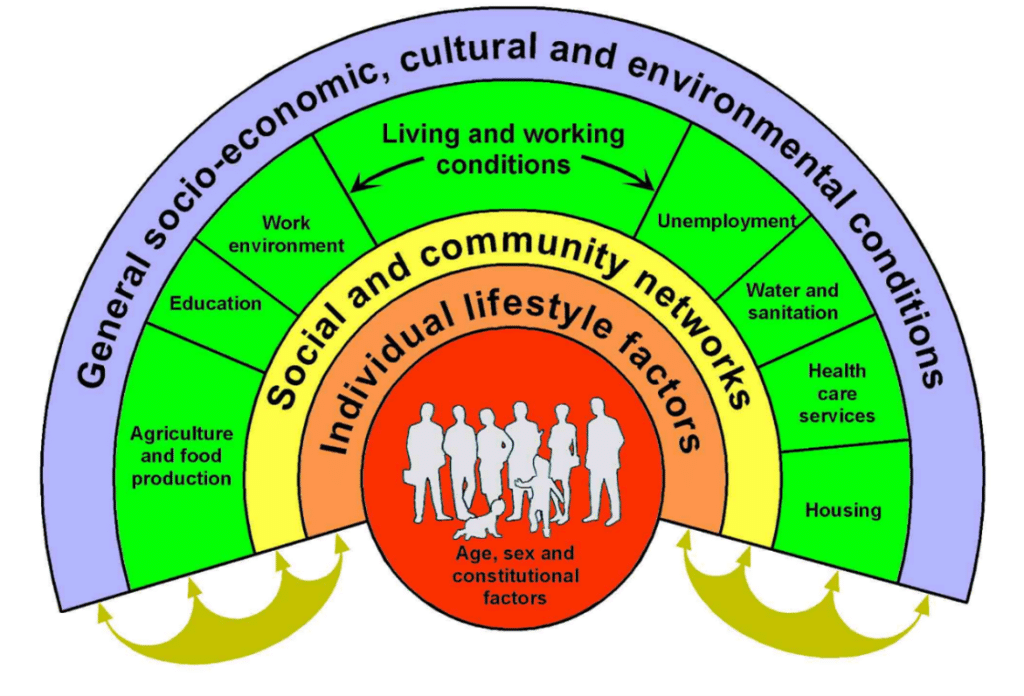
Source: Dahlgren and Whitehead, 1993 (adapted by University of Liverpool, 2023)
These essential building blocks of health are influenced by the policies and practices of a wide range of organisations. Transport, housing, fiscal and employment policies, although their primary remit is not health, can play a key role in reducing the unjust and preventable inequalities in health in our communities.
The Marmot review recommended that ‘social justice, health and sustainability’ should be at the heart of all policies. And that there should be a focus on the following 6 objectives, with the highest priority being given to the first objective:
- giving every child the best start in life
2. enabling all children, young people and adults to maximize their capabilities and have control over their lives
3. creating fair employment and good work for all
4. ensuring a healthy standard of living for all
5. creating and developing sustainable places and communities
6. strengthening the role and impact of ill-health prevention.
The South West has recently been identified as a Marmot Region, which provides an opportunity for key organisations and agencies across the South West to work with Sir Michael Marmot and his team to better understand the challenges within the Region, learn from other designated Marmot areas and Cities and agree a set of actions to help tackle inequalities.
Giving every child the best start in life is critical to the long-term health and wellbeing of our county. Improving outcomes for children, including through education and early years, is a top Marmot objective and a key priority for Devon County Council.
Working together for fair employment and good work for all, one of the six Marmot objectives, could make a very significant impact on health. Huge improvements in health and wellbeing can be made when local and national government, statutory organisations, businesses and the voluntary, community and social enterprise sector work collaboratively.
‘Anchor’ institutions can play a crucial role in improving the health and wellbeing of communities. An anchor institution refers to a large, stable organization that has a long-term presence and deep roots within a particular geographic community. Examples include local authorities, hospitals, universities, large businesses and the VCSE sector. These organisations typically have substantial physical infrastructure and human resources. What distinguishes anchor institutions is their commitment to the long-term well-being and development of the communities they serve. Given their stability, influence, and long-standing relationships, anchor institutions have the potential to act as catalysts for positive change. By collaborating they can address complex challenges and improve the overall quality of life in their communities through, for instance, the ways in which they recruit, invest and procure.
Figure 3.2 Anchor Institutions
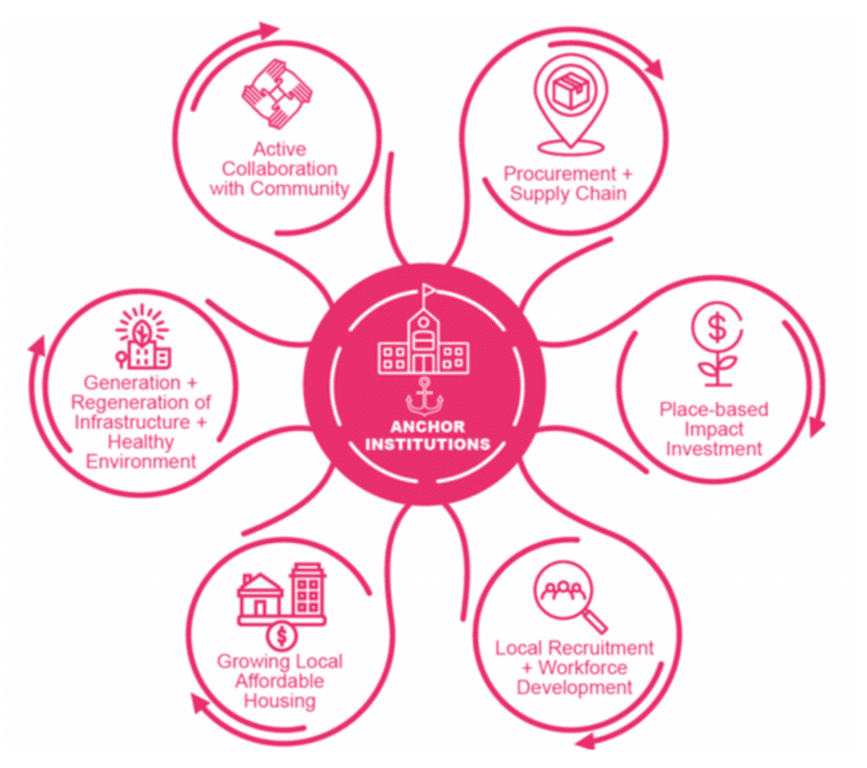
Source: Anchor institutions, Local Government Innovation Unit, 2022.
Mitigating and adapting to the climate emergency is arguably the most complex challenge we face. The climate emergency is a global health emergency that is contributing to increased illness and death and a widening of health inequalities. More extreme weather, rising sea levels, increasing carbon dioxide levels and rising temperatures have significant environmental impacts which in turn impact on health. Extreme heat, for instance, leads to increases in cardiovascular failure and heat-related illness and death. See figure 3.3 for an illustration of the impacts of climate change on health.
Figure 3.3 Impacts of Climate Change on Human Health
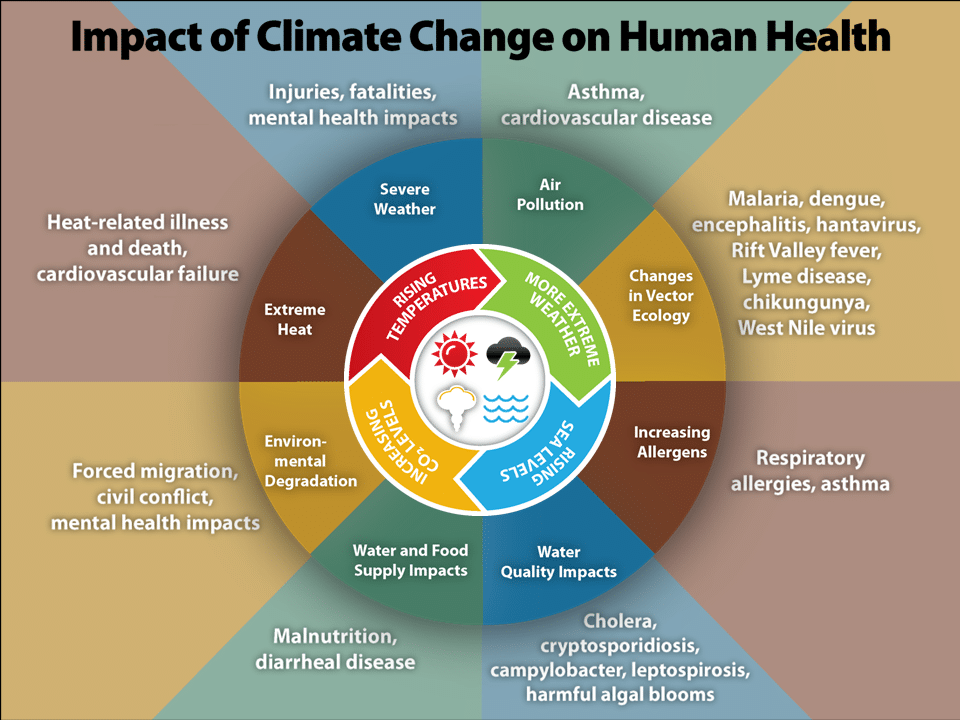
Source: ‘Impacts of Climate Change on Human Health’, Source: Patel, V. et al 2015. Disease Control Priorities, 3rd ed, vol 4, Washington, DC: World Bank. Adapted with permission from Dr. George Luber, Centre for Disease Control, USA.
The extent to which people are vulnerable to changes in the climate depends on three factors:
- exposure to climate health hazards (such as flooding or extreme heat or novel diseases)
- sensitivity to those hazards (e.g. people over 65 have increased sensitivity to extreme heat)
- their ability to adapt and cope with the consequences.
There is a clear need to proactively adapt as climate change affects our critical infrastructure (e.g. transport and communication networks), community assets (e.g. schools, hospitals, parks), homes and the wider environment in which we live.
Many actions to mitigate climate change also have health co-benefits, see Figure 3.4.
Figure 3.4 Health and climate: co-benefits
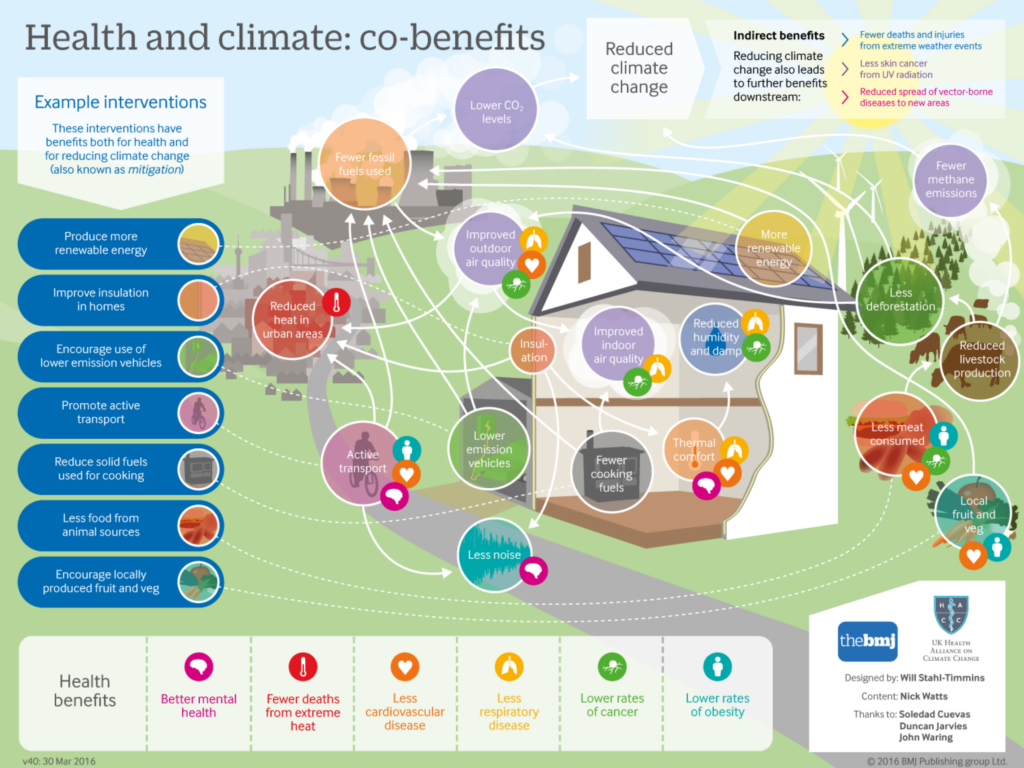
Source: British Medical Journal, 2016;352: i1781
Place-Based Approach: Social and community networks are also critical to our health and wellbeing. There is a growing body of evidence about how greater community control, inclusion and participation can improve community and individual health and wellbeing. Improved social support, strong networks and communities that feel empowered and involved are important foundations that provide a bedrock for improving skills, job prospects, self-esteem, cohesion and access to services and health outcomes. (PHE, 2019, ‘Health inequalities: Place-based approaches to address health inequalities’).
Devon’s key challenges that require us to take a ‘health in all policies’ approach:
Social and economic inequalities in Devon already exist and the cost-of-living crisis is making this worse as it affects people who are already struggling the most. People in rural areas face additional cost-of-living pressures due to higher energy, food and transport costs and the difficulties with digital connectivity.
Many employers in Devon are finding it difficult to hire people, particularly in health and social care, because pay is often low, and housing is expensive and in limited supply. There are also insufficient people in the job market to fill vacancies and a skill gap: skill levels are much lower in some parts of Devon than in others.
The businesses on which Devon depends, like construction, tourism, hospitality, and retail, are the ones most likely to suffer in the economic crisis: this includes reductions in discretionary spending and significant slowing in construction.
The financial situation is curtailing the ability of Public Sector partners and the Voluntary, Community and Social Enterprise (VCSE) sector to respond to increasing levels of need, particularly among the most vulnerable. A survey of Devon households in October ‘22 found that 29% are food insecure and 36% were planning to keep their heating switched off over the winter (2022/23) (Transform research, Jan 2023). Cold, damp homes and a lack of access to food puts people already vulnerable at higher risk of illness and death. There is also a risk that if the preventative work of statutory and VCSE organisations is significantly reduced the burden on frontline statutory services will increase even more.
People living in areas of high deprivation within Devon and many people with protected characteristics already have poorer health and wellbeing outcomes. The pandemic has exacerbated the mental health difficulties faced by young people and created new challenges for people living with ‘Long-Covid’. Devon is also responding to the specific needs of refugees and asylum seekers.
The Devon system has produced a 5 year integrate care strategy called the Joint Forward Plan and this captures the key challenges facing Devon and includes some of the key wider determinants that are impacting on the health and wellbeing of Devon residents and contributing to the health inequalities that exist in Devon. Key challenges identified includes, climate change, housing quality and affordability, economic resilience and education, training and employment opportunities, workforce availability and wellbeing. Having these wider determinants included within the plan provides an opportunity for the system to work collectively on these key issues over the coming years.
Local approaches to addressing the wider determinants of health:
The following two examples are of cross sectoral partnerships that are acting together to create fairer, healthier and more resilient and prosperous communities across Devon.
Energy Saving Devon (Energy Saving Devon) is a partnership of community energy groups collaborating to tackle the climate crisis and alleviate fuel poverty. Their vision is to work together to make every house in Devon regenerative, healthy to live in and affordable to run, in line with the Devon Carbon Plan. Their work focuses on giving the most help to those with the highest level of need whilst helping everyone move towards low carbon, energy efficient forms of living. Advice and guidance on how to reduce heat loss and improve energy efficiency is therefore available to everyone. Working with the NHS, local authorities and wider partners this network of community energy organisations have provided vital support during the cost-of-living crisis.
The Devon Food Partnership was established to enable collaboration and communication between food stakeholders across the county. It aims to promote strategic, whole-system change across the county with the ambition that healthy, sustainable, and affordable food can be made accessible to all. A food strategy has been written to bring everyone from farmer to consumer and business owner to volunteer together, across all sectors, to promote the kind of whole-system changes that are needed for both planetary and human health. It aims to address the stark inequalities in access to healthy, affordable food that are seen in Devon, whilst promoting a food and farming sector that is thriving and sustainable and supports the future resilience of our communities.
Reflections:
We know the conditions in which we are born, grow, live, work and age are key determinants of our life expectancy and healthy life expectancy. Addressing the ‘causes of the causes’ of ill health is vital to tackle the growing health inequalities that exist nationally and within Devon. With the South West recently being named a Marmot Region it is important we learn from other designated Marmot areas and work together with wider system partners, including the voluntary and community sector but also importantly with communities and residents to ensure the right building blocks are in place to promote and protect people’s health. The inclusion of some of these challenges within the Joint Forward Plan will require system partners to work more collaboratively to address these issues and importantly be accountable for agreed outcomes to measure improvements.
Recommendations:
- Devon Integrated Care Partnership should work together to realise the potential they have as anchor institutions to improve the lives of local people and reduce health inequalities, drawing on evidence of the impact of this approach from other areas (https://doi.org/10.1016/S2468-2667(23)00059-2).
- Devon Health and Wellbeing Board to consider the impact of the climate emergency on health and equity, through the production of a joint strategic needs assessment; The board should review, adopt and monitor the partnership’s climate change mitigation and adaptation plans and the opportunities they present to create a fairer, healthier, more resilient and more prosperous society.
- Public Health Devon to actively work with system partners to support the delivery of the agreed Joint Forward Plan objectives and actions in relation to taking the wider determinants of health.
- Public Health Devon to actively participate in the Marmot Region work programme and ensure learning is shared with Integrated Care Partnership.
- The Devon Food Partnership and the Energy Saving Devon partnership utilise every opportunity to address health, equity and the climate emergency through their collective programmes.
4. Primary prevention

Everyone deserves to live a long happy life in full health. However, far too many people lose what should be healthy years, through illness and disease and much of this premature ill health and early death can be attributed to behaviours such as tobacco smoking, poor diet, harmful alcohol use and physical inactivity.
There is a pressing need to prioritise the primary prevention of these risks, acting upstream to avoid the loss in health and wellbeing experienced by so many of Devon’s residents.
Post Pandemic we know that rates of childhood obesity have risen sharply, and inequalities have widened. Smoking remains stubbornly high among those living in more deprived areas. Alcohol-related hospital admissions and deaths have escalated, and rates of harmful drinking have increased. Physical activity levels also remain low and appear to have declined during the pandemic (Addressing the leading risk factors for ill health – The Health Foundation).
The Global Burden of Disease ranks the top 20 causes of Ill health in Devon and as you can see in figure 4.1, Neoplasms (cancers) followed by cardiovascular disease are the top two causes. Most of the preventable risks to health outlined in the Global Burden of Disease have multiple, interrelated causes which cluster in socioeconomically disadvantaged areas.
Figure 4.1, Top 20 ranked causes of ill health in Devon, 1990 and 2019, measured in disability adjusted life years (DALYs) per 100,000 population
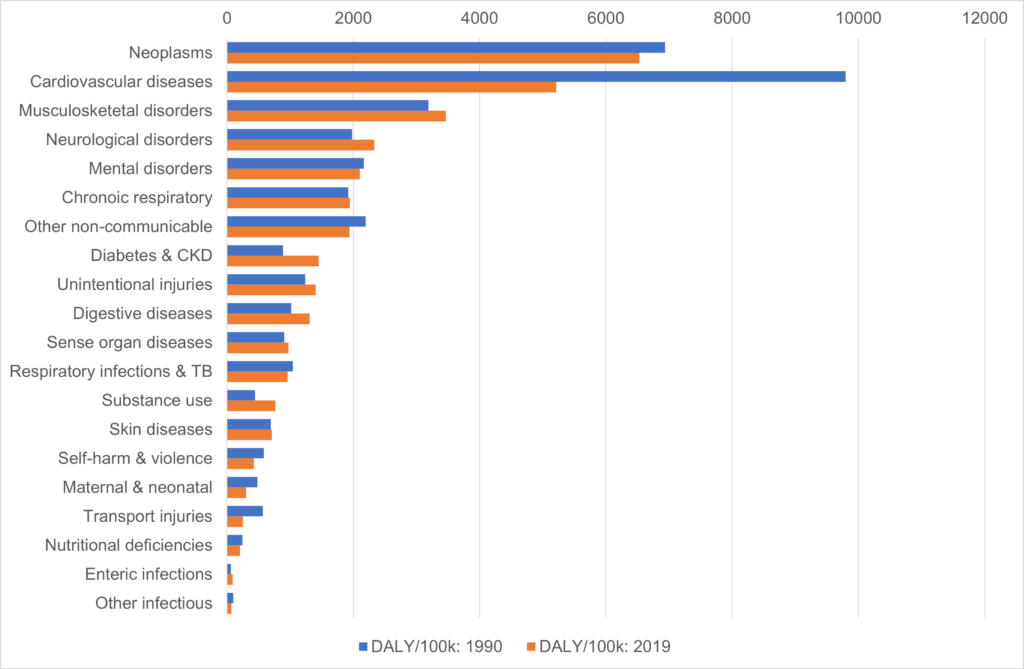
Source: Global Burden of Disease, GBD Compare, Institute of Health Metrics and Evaluation, 2023 VizHub – GBD Compare (healthdata.org)
Primary prevention acts on modifiable risks seeking to prevent the avoidable associated ill health and early death that are unequally distributed through society. Approaches to primary prevention vary from those that focus on individual actions, personal responsibility and choice; seeking to help people change their behaviour through a range of psychologically based interventions and campaigns, to broader population-focussed approaches which seek to address the social, political and economic conditions that act directly on people’s health.
For example, when considering how to address dietary risks, individual approaches include a dietician or weight management professional working to help a person plan how to change what they eat. These can be contrasted with population approaches targeted at community or setting level, such as developing community based social supermarkets to improve the access and affordability of healthy food, improvements in school catering, or a junk food advertising ban on public transport, as seen recently in London (Changes in household food and drink purchases following restrictions on the advertisement of high fat, salt, and sugar products across the Transport for London network: A controlled interrupted time series analysis | PLOS Medicine) with a shift to a healthier food advertising policy, also planned in Wales (gov.wales/sites/default/files/publications/2019-10/healthy-weight-healthy-wales_0.pdf).
Figure 4.2 Foresight systems map for obesity. The full obesity system map with thematic clusters
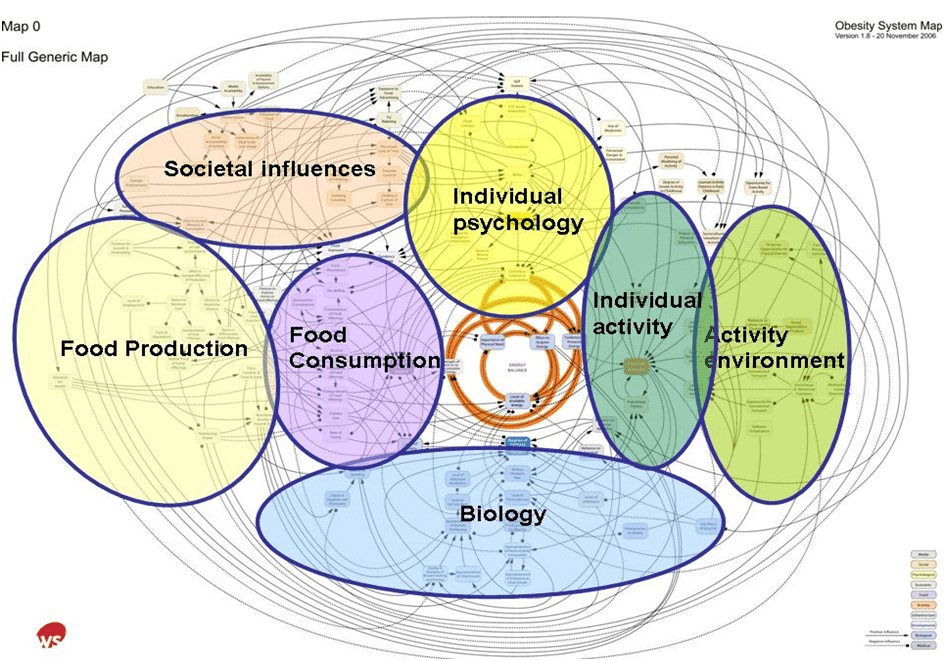
Source: Tackling obesities: future choices report, Government Office for Science, 2007 Tackling obesities: future choices – GOV.UK (www.gov.uk)
There has been a growing recognition that everyday behaviours are driven and shaped by a dynamic web of interrelated factors within a complex adaptive system. This makes individual efforts to change seemingly modifiable behaviours much more difficult, if concurrent work to address these conditions is missing. As Sir Michael Marmot explained in 2015
‘The fact is that the conditions to which we are exposed influence our behaviour. Most of us cherish the notion of free choice, but our choices are constrained by the conditions in which we are born, grow, live, work and age’. (The health gap: the challenge of an unequal world – The Lancet)
Over recent years there has been much acknowledgement that the causes of behaviours are complex, but research around excess weight (Understanding how local authorities in England address obesity: A wider determinants of health perspective – ScienceDirect) and the other leading risk factors (Addressing the leading risk factors for ill health – The Health Foundation) has shown that the balance of action across government and many local areas has remained in favour of individually oriented approaches. This is hardly surprising, not least because individualised approaches support those who ask for help and they are popular with the public, for example smoking cessation services or weight management services. Individual approaches are also easier to describe and measure and so have been researched extensively; they fit in with clinical treatment models of care and are more actionable, as they do not need to involve so many stakeholders or organisations. Time frames for individual approaches are also shorter, with action to address social contexts requiring a sustained, long-term commitment. We need to review the balance in the approach.
The scale of challenge means that we need to look in depth at our communities and at the wider systems that directly impact on health, and work collaboratively with communities to develop multi-level programmes of work, employing Systems Thinking approaches to study and understand the interrelationships between factors before seeking the best places to intervene.
As risk factors cluster in communities, approaches may need to reflect this, clustering to effect change where we can gain most impact on complex, interwoven behaviours; joining up actions where that makes sense and ensuring that the principle of “proportionate universalism” (Fair Society Healthy Lives (The Marmot Review) – IHE (instituteofhealthequity.org)) is applied, which involves spreading resources across all communities to improve everyone’s health but with a scale and intensity proportionate to need, in order to close the life expectancy gap.
A joined-up response to clustered risks may also be required within individual approaches, as we know that many of us struggle with a range of health risks at the same time and insight work here in Devon (Our Five-year Integrated Care Strategy – One Devon) has heard from residents who say they want to be supported as a whole person rather than as a set of separate risks or conditions. This need for alignment is recognised in the forthcoming national Major Conditions strategy which identifies “multi morbidity prevention” as a fresh approach in supporting people to address health risk behaviours.
A strengthened System understanding of the contribution of social, economic and environmental factors and commercial determinants, should lead to both a reset in the balance of approaches to primary prevention but also an opportunity to reframe individual support to adopt a more compassionate approach. Compassionate approaches seek to eliminate stigma and shame through shifting blame away from individuals, helping people navigate the unfair environments they live in and focus on health gains relative to their own lives and aspirations.
With a re-balanced approach, individual support will sit within a wider programme of complementary population-based action at community level and place. Such multi-level programmes have the chance to shift a larger proportion of the population into the lower risk category, rather than approaches that focus entirely on the highest risk individuals, as depicted in the figure below.
Figure 4.3 The Bell-Curve Shift in Population Health
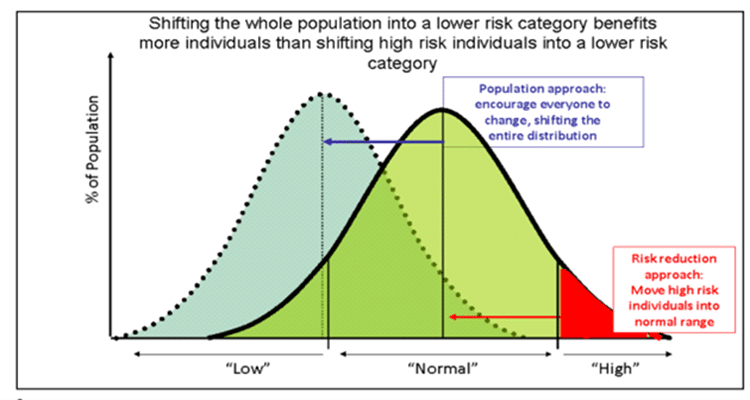
Source: Rose G. Sick individuals and sick populations. International Journal of Epidemiology. 1985; 12:32-38
There are of course important factors that require national and global action which are beyond a local area’s sphere of influence, such as the role of commercial determinants driving marketing and pricing practices and the role of national legislation, e.g smoking ban in public places, however there is much that can still be done at local level and at place.
Case study
The Smokefree Devon Alliance, takes a co-ordinated, multi-agency response to tobacco control. Work focusses particularly on preventing harm to babies and children, including smokefree pregnancies, families, homes and play parks to reduce exposure to second hand smoke. Education on smoking is delivered through schools, action to reduce illegal tobacco, which is cheap and accessible within communities is led by Trading Standards and collective work to de-normalise smoking in society is delivered through campaigns and smokefree policies. Working individually to help smokers quit, forms an important part of the overall programme and investment into treating tobacco dependence within secondary care by NHS England recently, has increased the commitment within hospitals and NHS trusts. With sustained co-ordinated effort, maternity care around treating tobacco dependence has been transformed over the past five years and now all women are provided with effective support
Taking a multi-faceted approach to tobacco control in this way, combining population and individually focussed interventions has created a comprehensive approach to prevention of harm from tobacco and combined with national legislation, can be credited with the steady upward trend in the proportion of Devon’s residents living smoke free lives.
Primary Prevention Opportunities
Across Devon we have a range of county and place-based partnerships co-ordinating primary prevention action. Some of this action is topic focussed, acting at county or locality level, such as the Devon Food Partnership, the Devon Alcohol Harm Reduction Partnership and the One Northern Devon Healthy Weight, Physical Activity & Movement Group. We also have condition-specific groups such as the Cardiovascular Disease Prevention group which combines work across primary and secondary prevention, focussing also on identification initiatives, given the largely symptom-free nature of high blood pressure for example.
Alternatively, there are place-based partnerships such as One Northern Devon and other Local Care Partnerships, which seek to utilise the strengths and assets within a place to join and align resources to improve health and wellbeing.
In each of these partnerships, a wide range of organisations, community members and stakeholders contribute to a programme of multi-level action. Where partnerships work effectively, roles and contributions are clarified, resources and goals are aligned, and the collective efforts and collaborative working achieves much more than the sum of the individual contributions.
If place-based and topic-focussed partnerships work together there is an opportunity to ensure that primary prevention action is co-designed and driven by communities, that finite available resources are maximised, and that collective action achieves a greater scale of demonstrable health gain across Devon’s population.
Reflections
The challenge will be finding appropriate ways to measure and demonstrate impact in the short and medium term, given the longer timescales required to effect change on the conditions that drive health risk behaviours. Impact measures that can demonstrate progress in the right direction will help to build confidence in a re-balanced approach, which in time, with sustained effort, will demonstrate the outcomes we all seek; longer, healthier and happier lives for everyone in Devon.
Recommendations
- Public Health Devon and Devon Integrated Care Partnership to work collaboratively with communities within multi-agency alliances, to develop and refine multi-level programmes of action on the leading modifiable risk behaviours (tobacco, food, excess weight, alcohol, physical inactivity), ensuring there is an appropriate mix of individual and population level approaches to make an impact at pace and scale.
- Public Health Devon to work with stakeholders in Devon Integrated Care Partnership to develop and implement a programme of professional development to upskill the workforce in compassionate, health gains approaches to healthier weight to destigmatise individual behavioural change interventions, promoting confidence and emotional wellbeing.
Public Health Devon to work with system partners to test place-based approaches to drive community-based prevention action. These should be designed with and informed by local communities, utilise community assets and act on clustered risks, utilising proxy measures to demonstrate impact in the short to medium term.
5. Secondary prevention

Secondary prevention involves systematically detecting the early stages of disease and intervening before full symptoms develop. The failure to detect the early stages of disease will lead to higher levels of ill health, disability, and premature death, which not only has a considerable human impact, but also increases the demand for health and care services and impacts financially through increased healthcare costs and the wider economic impacts of ill health.
One way of considering the impact is to look at changes in disability adjusted life years (DALYs). A DALY is the loss of the equivalent of one year of full health. DALYs for a disease or health condition are the sum of the years of life lost to due to premature mortality (YLLs) and the years lived with a disability (YLDs) due to prevalent cases of the disease or health condition in a population.
An analysis of DALYs per 100,000 population in Devon (figure 4.1) reveals that the causes of ill health and premature death with the greatest impact in Devon are neoplasms (cancers) and cardiovascular disease. Three other causes have seen significant increases in their rank and overall impact over recent years. These are substance use disorders, neurological disorders, and diabetes/kidney disease. This chapter focuses on these five causes of premature death, poor health and disability, and looks at the secondary prevention opportunities available to reduce their impact.
The following subsections look at these five causes of particular concern in Devon and the secondary prevention opportunities relating to them.
a) Neoplasms
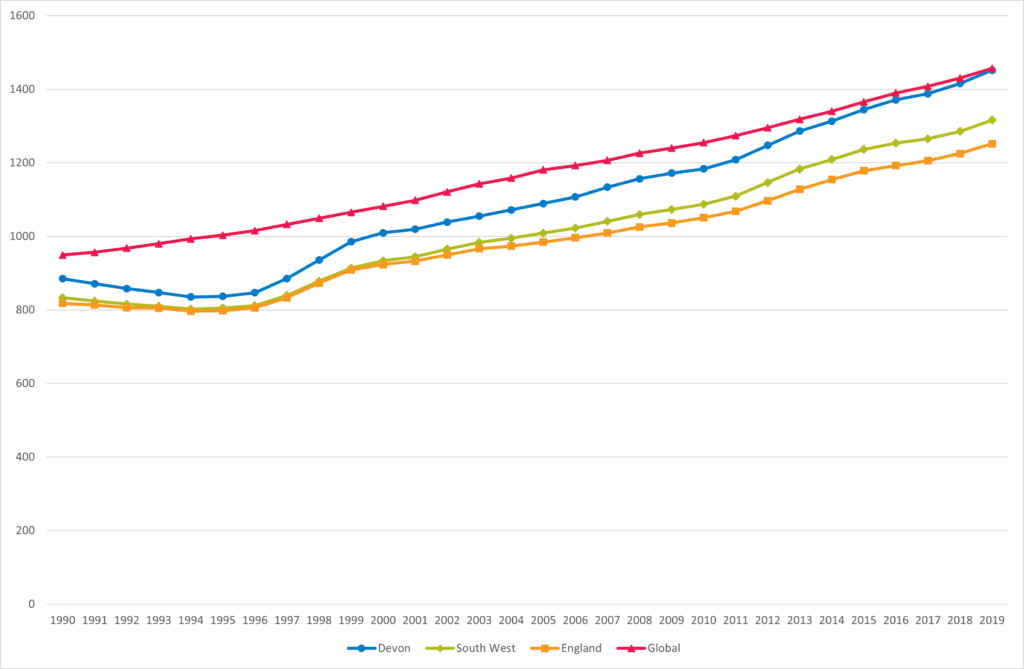
Deaths and disability caused by neoplasms (cancers) has been increasing since 2014 with higher levels compared to the South West, England and the global position. Neoplasms are the largest contributor to ill health and premature death in Devon. Significant inequalities also exist with higher levels of certain cancers with 30,000 extra cases of cancer in the UK attributable to social and financial deprivation (Cancer Research UK – Science blog) with higher mortality rates in more deprived areas.
Figure 5.1, Trend in Disability Adjusted Life Years per 100,000 for Cancer in Devon, 1990
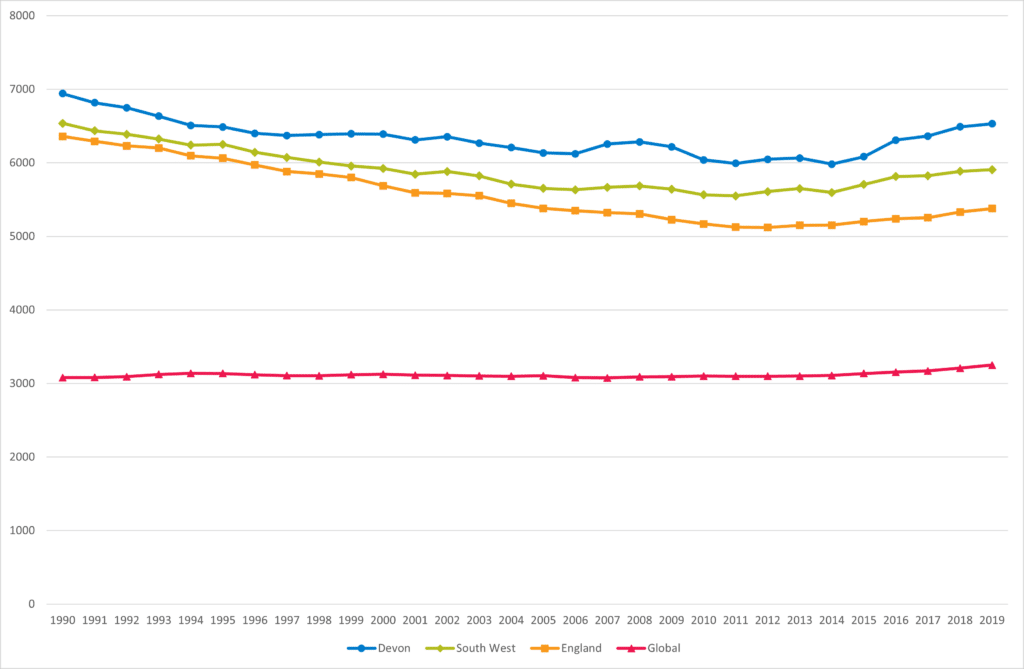
Source: Global Burden of Disease, GBD Compare, Institute of Health Metrics and Evaluation, 2023 VizHub – GBD Compare (healthdata.org)
Secondary Prevention opportunities
The early identification of cancer greatly improves the chances of survival. A numbering system is used to divide cancers into four stages, with stage 1 indicating the cancer is contained to a single organ, stage 2 into surrounding tissues, stage 3 indicating greater spread into surrounding tissues and lymph nodes, and stage 4 indicating spread to other organs of the body. Around 52.3% of cancers detected in England, and 54.7% in Devon were at stage 1 or 2, with higher proportions detected at stages 1 and 2 in more deprived areas (Public Health Outcomes Framework – Data – OHID (phe.org.uk)):
The main secondary prevention approaches are:
- Cancer screening: NHS screening tests (NHS screening – NHS (www.nhs.uk)) are available for cervical screening (available to all women aged 25 to 64), breast screening (available to all women aged 50 to 70 with self-referral available to women over 70, and bowel screening (home screening kits available to everyone aged 60 to 74). The Public Health Outcomes Report reveals variation in cancer screening with those living in more deprived areas having lower levels of uptake. Cancer Research UK have highlighted the importance of understanding and breaking down barriers to screening, including stigma, misinformation and practical barriers (Cancer Research UK – Science blog).
- Cancer awareness campaigns: educating and enabling people to identify the potential early signs of cancer by raising awareness of symptoms is also important. The NHS A to Z guide (Health A to Z – NHS (www.nhs.uk)) is a useful practical guide to symptoms and conditions and what to do about them. Campaigns aimed to increase public awareness of different cancers run throughout the year and are summarised here (Cancer awareness calendar | Cancer Research UK).
b) Cardiovascular disease
Premature Deaths and disability caused by cardiovascular disease (such as heart disease and stroke) decreased significantly between 1990 and 2010 but has been gradually increasing in recent years. The burden of cardiovascular disease is greater in Devon compared to the South West, England and the global position. Significant inequalities exist in relation to ill health and disability caused by cardiovascular diseases, with the Kings Fund Cardiovascular disease in England report (Cardiovascular disease in England | The King’s Fund (kingsfund.org.uk)) highlighting that people living in the most deprived areas were four times more likely to die prematurely from cardiovascular disease as those living in the least deprived areas, along with higher risk in South Asian and Black ethnic groups.
Figure 5.2, Trend in Disability Adjusted Life Years per 100,000 for Cardiovascular diseases in Devon, 1990 to 2019
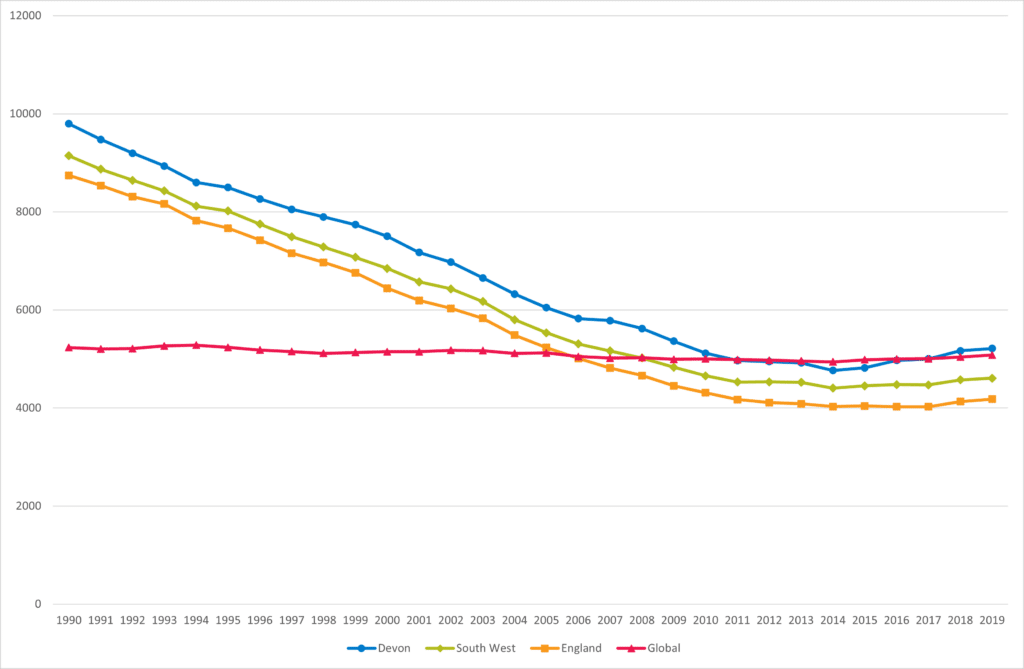
Source: Global Burden of Disease, GBD Compare, Institute of Health Metrics and Evaluation, 2023 VizHub – GBD Compare (healthdata.org)
Secondary Prevention opportunities
Secondary prevention approaches for cardiovascular diseases include:
- Hypertension case finding: hypertension (also known as high blood pressure), is usually defined as having a sustained blood pressure of 140/90mmHg or above. Around half of people with hypertension are undiagnosed due to not having their blood pressure tested, increasing their risk of heart disease or stroke, which could be greatly reduced through lifestyle changes and/or medication. Blood pressure monitoring in community pharmacy settings followed by home based monitoring is highlighted by NHS England (NHS England » Cardiovascular disease high impact interventions) as a high impact intervention to reduce the impact of cardiovascular disease, with the potential to increase the identification of hypertension, reduce the burden on health services and promoting healthier behaviours, saving both the NHS and local authorities money.
- Cholesterol search and risk stratification: risk stratification refers to methods of grouping people according to health risks, with the intention of identifying those of high or increasing risk who may require further support. This is one of the tools available within Population Health Management, a set of data-driven approaches to target preventive interventions to improve the health of the population. Cholesterol search is another high impact intervention highlighted by NHS England (NHS England » Cardiovascular disease high impact interventions) which uses existing healthcare data to find cases with high- risk conditions, those who have had a recent acute cardiovascular event, or those with a family history to target support to manage and reduce cholesterol. This is a low-cost intervention, adaptable to local systems, with the potential to save lives, reduce hospital admissions and cut costs. Data-driven methods to identify and stratify risk across multi-conditions are cost effective and possible through the One Devon Dataset, a linked dataset combining health, care and wider population data for Devon.
- NHS Health Check: health checks are available to those aged 40 to 74 in England and can spot the early signs of stroke, kidney disease, heart disease, type 2 diabetes or dementia, and are another high impact intervention highlighted by NHS England (NHS England » Cardiovascular disease high impact interventions). Around one in every four attendees are identified as being at risk of cardiovascular disease, leading to recommendation of lifestyle changes, or, if required, medication. Attendance at health checks is also associated with a reduced risk of hospital admissions and deaths relating to cardiovascular disease. A targeted approach should be used in Devon to ensure that health checks are made available and promoted in more deprived areas and to groups with greater risk of cardiovascular disease.
c) Substance use
Substance use disorders include alcohol and substance use disorders. Levels of ill health and premature death from these disorders is above the global average and are significantly higher than the levels seen in the 1990s and 2000s. This is also reflected in increases in deaths of despair, which cover deaths from suicide, alcohol and drug use, which have increased significantly over the last 20 to 30 years, and which recent evidence indicates experienced a further increase during the Covid-19 pandemic (Increases in ‘deaths of despair’ during the COVID-19 pandemic in the United States and the United Kingdom – PMC (nih.gov)). Considerable health inequalities exist in relation to substance use disorders, with alcohol and drug related problems, hospital admissions and deaths significantly higher in more deprived communities.
Figure 5.3, Trend in Disability Adjusted Life Years per 100,000 for Substance Use Disorders in Devon, 1990 to 2019
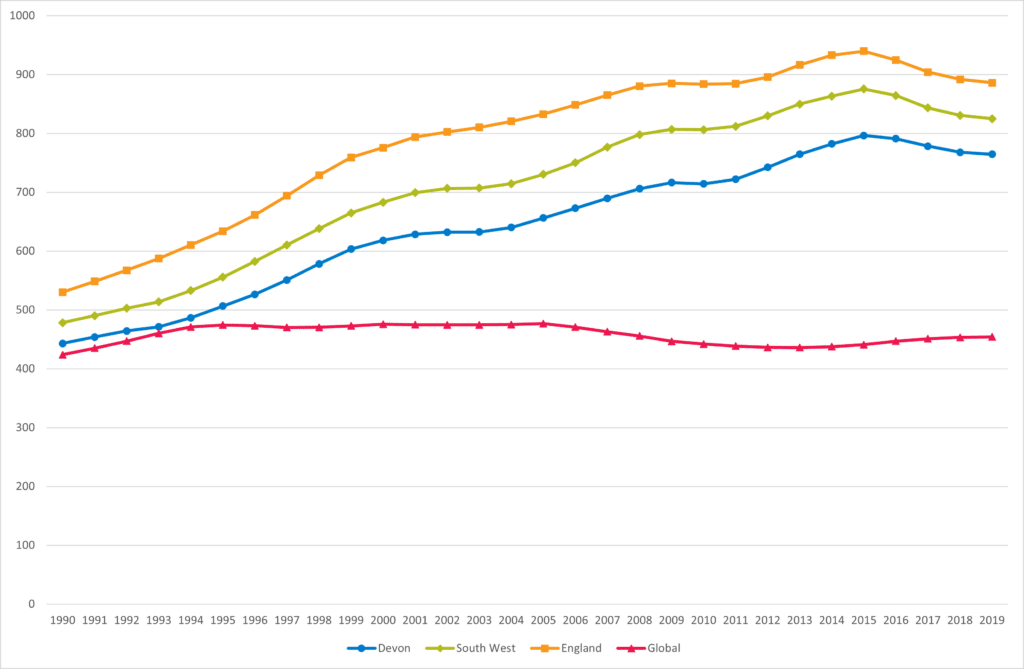
Source: Global Burden of Disease, GBD Compare, Institute of Health Metrics and Evaluation, 2023 VizHub – GBD Compare (healthdata.org)
Secondary Prevention opportunities
The main mechanism for the early detection of substance use issues is the Making Every Contact Count (MECC) programme. MECC is an approach to behaviour change that uses the millions of day-to-day interactions that organisations and individuals have with other people to support them in making positive changes to their physical and mental health and wellbeing. In relation to substance misuse, this involves supporting patients with mild substance use problems or hazardous drinking and drug use patterns that may not meet diagnostic criteria for substance abuse and dependence, as well as helping with wider issues that may impact on health such as social isolation, managing debt, or in tackling housing issues. Simple structured questions around substance use (MECC Link) enable brief interventions to be made. Health checks (see section B) also provide an opportunity to discuss substance use and behaviour change.
d) Neurological disorders
Neurological disorders (Alzheimer’s disease and other dementias, Parkinson’s disease, epilepsy, and multiple sclerosis) are increasing. This increase is largely driven by Alzheimer’s disease and other dementia), which in turn is influenced by an ageing and growing population in Devon. The burden or neurological conditions in terms of premature death, ill-health and disability in Devon is greater and growing more rapidly than the South West, England and the global position.
Figure 5.4, Trend in Disability Adjusted Life Years per 100,000 for Neurological Disorders in Devon, 1990 to 2019
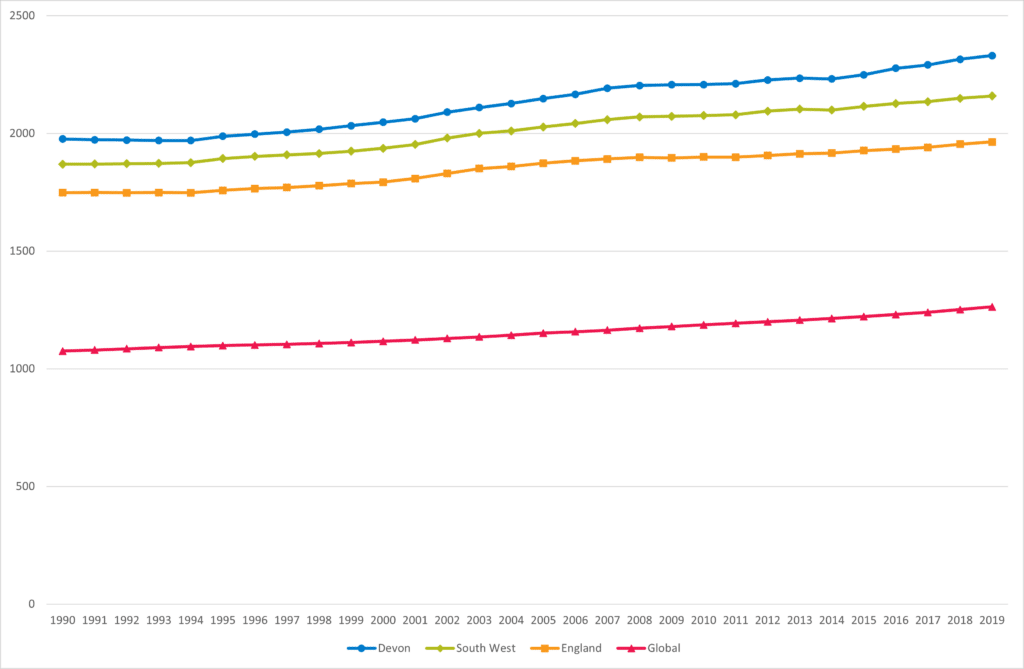
Source: Global Burden of Disease, GBD Compare, Institute of Health Metrics and Evaluation, 2023 VizHub – GBD Compare (healthdata.org)
Secondary Prevention opportunities
Whilst the progression of dementia cannot be reversed, it can be slowed with early detection and appropriate support and intervention. However, in the early stages dementia can go undiagnosed. In Devon, according to the Public Health Outcomes Framework, general practice dementia registers account for around 55.6% of those expected to have dementia, which is lower than the national average (62.0%). A timely diagnosis enables people living with dementia, their carers and healthcare staff to plan accordingly and work together to improve health and care outcomes. The Alzheimer’s Society has made a number of recommendations to improve the uptake of dementia diagnosis (Increasing access to a dementia diagnosis | Alzheimer’s Society (alzheimers.org.uk)), including case finding activities, streamlining pathways and targeting under-represented communities. Memory Cafés provide spaces for comfortable social interaction for people experiencing memory loss and their families to connect and build new support networks. The Devon Memory Café Consortium (https://dmcc.org.uk/) brings together memory cafés across Devon and includes links to local cafés. Further details are dementia advice and support are also available on Devon County Council website (Worried about your memory? Access support and advice in Devon | Devon County Council).
e) Diabetes and kidney disease
Premature death and disability relating to diabetes and kidney disease is on the increase across the world. Levels have increased from below the global average in Devon during the 1990s and 2000s to levels comparable with the global average and well above the South West and England average today. Whilst this pattern is largely driven by increases in diabetes, increases in chronic kidney disease has also been apparent. Changes in diet, obesity and physical activity over the last 30 years are major factors in these increases. Significant health inequalities also exist with higher levels of these conditions, hospital admissions and deaths in more deprived communities. Ethnic inequalities are also evident with people from Black African, Caribbean and South Asian (Indian, Pakistani, Bangladeshi) backgrounds at higher risk of developing type 2 diabetes from a younger age.
Figure 5.5, Trend in Disability Adjusted Life Years per 100,000 for Diabetes and Kidney Diseases in Devon, 1990 to 2019
Source: Global Burden of Disease, GBD Compare, Institute of Health Metrics and Evaluation, 2023 VizHub – GBD Compare (healthdata.org)
Secondary Prevention opportunities
Secondary prevention opportunities relating to diabetes include:
- Structured education: Diabetes self-management education are designed to help people with diabetes stay healthy and prevent complications that would severely impact their health and quality of life as well as increasing costs. These courses which integrated self-managed and directly learning provide people with the skills and confidence required to manage their own condition. Structured education is identified as a high impact intervention (NHS England » Diabetes high impact interventions) with the dose adjustment for normal eating programme (DAPNE) estimated to save around £2,200 per patient treated over 10 years and reduce emergency treatment costs by two thirds for related complications.
- NHS diabetes prevention programme: The NHS diabetes prevention programme (NHS England » NHS Diabetes Prevention Programme (NHS DPP)) focuses on detecting the precursors to diabetes so lifestyle changes can be put in place before full symptoms develop. The programme involves both face-to-face elements, including direct advice, and digital elements, integrating wearable technologies to monitor exercise and related apps. By identifying at an early stage the risk of developing type 2 diabetes is reduced by over a third for those completing the programme.
Nine diabetes care processes: The ongoing management of diabetes within primary care is another important high impact intervention which reduces the likelihood of exacerbations, complications and premature death. These nine NICE recommended processes (NHS England » Diabetes high impact interventions) involve the measurement of various factors including weight/BI, blood pressure, HbA1c, smoking status and cholesterol. The completion of these processes reduces the risk of premature death, hospital admissions, amputations and diabetic retinopathy.
Reflections
The ethical and economic case for secondary prevention is compelling. Detecting health conditions in their early stages to put effective treatments in place, saves lives, money, reduces demand on health and care services and improves the quality of people’s lives. This section has set out the five causes of ill health, disability and premature death in Devon which are of the greatest concern, either due to overall impact, or increases in recent years. For each of these well evidenced and cost-effective programmes and interventions are available to address this and are in place in Devon. Given the immediate and longer-term challenges our local health and care system is facing, it is essential that we make the most use of our collective resources to enhance and scale up our secondary prevention programmes to improve early detection and reduce inequalities in access and outcome.
Recommendations
- Through the Population Health Management programme, the Devon Integrated Care System should implement a range of data-based approaches for case finding for avoidable conditions or to improve outcomes. These methods should focus on detecting the precursors and early stages of disease, design preventive interventions and monitor their impact.
- Following the success of the Devon mass vaccination inequalities cell through the Covid-19 pandemic, the application of a multi-disciplinary inequalities cell approach to secondary prevention programmes to drive action around community engagement and targeting and reducing inequalities.
6. Tertiary prevention

Tertiary Prevention is needed when an individual has already developed declining health and it is the most expensive level of prevention as the individual requires health and care treatment and support. It is about restoring an individual’s health to the most optimal that can be achieved and likely to involve reducing symptoms and disability.
Living and ageing well approaches and strategies need to focus on evidence-based disease management, rehabilitation, reablement, intermediate and integrated care and crisis management. Tertiary prevention also needs to support the wider determinants of health including warm and safe homes to prevent deterioration of long-term conditions and adequate nutrition (and hydration) which have been adversely impacted by the current cost of living.
Prevention Opportunities
- Ageing well including dementia risk reduction
The earlier in life that healthy changes are made, the greater the likelihood of delaying the onset of dementia, disability and frailty. The whole system needs to work together to identify those at greater risk and support population and community-level initiatives to enable people to be independent, healthy and active in later life.
Prevention must be integrated into services so that professionals can help recognise early signs and refer to dementia and frailty support services and interventions should be tailored to the individual.
- Preventing digital exclusion
Digital access and skills are a wider social determinant of health and to reduce health inequalities it is important to mitigate against digital exclusion and to build trust and relationships with poorly served groups by co-designing digital health and care services. For example, supporting people to try out different devices and assistive technologies, encouraging community involvement as digital health champions.
This can be supported by improving digital and basic literacy skills in the local community and develop digital health hubs to improve inclusion. For example, via social prescribing, and working with local community VCSE organisations.
- Preventing loneliness and social Isolation
We saw throughout the Pandemic how communities came together to support vulnerable families and individuals through supplying essential food parcels but also companionship. Asset-based community development can help address loneliness at a neighbourhood and ward level as older people and individuals in poor health spend more time in, and often feel more committed to their neighbourhood. Breaking down areas at neighbourhood level can also be more manageable and allow effective targeting of initiatives and enables outreach efforts.
There are many existing programmes that identify individuals who are experiencing loneliness and targeting people at risk of loneliness, including social prescribing to connect them to programmes and support.
As part of the building blocks for health and wellbeing gateway services such as transport, technology, spatial planning, and housing, should make it easier for communities to come together to identify options for affordable and accessible transport; age-friendly driving and parking and should consider social networks as a health determinant.
The integrated system should work in partnership to offer direct interventions to reduce loneliness, these may be focussed on supporting and maintaining relationships, supporting new connections or psychological approaches. This could include support group activities such as lunch clubs and walking groups, one-to-one approaches like befriending schemes, access to psychological support for people for whom loneliness is part of broader mental health issues.
- Falls prevention and management
People aged 65 and older have the highest risk of falling, with 30% of people older than 65 and 50% of people older than 80 falling at least once a year. The human cost of falling includes distress, pain, injury, loss of confidence, loss of independence and mortality. Falling also affects the family members and carers of people who fall (Falls and fractures: consensus statement and resources pack – GOV.UK (www.gov.uk)).
Fractures and hospitalisation occur in around 5% of adults with a history of falls living in the community and falls are estimated to cost the NHS more than £2.3bn per year.
Falls prevention programmes that identify individuals at risk of falls using a multifactorial risk assessment and providing timely and evidence-based tailored interventions to reduce falls and fracture risk across the life course remain important. Interventions to prevent falls should be tailored to the needs of the individual. Examples can include strength and balance exercise programmes (1:1, group or virtual), multifactual falls assessment when discharging patients, home environment modifications ranging from simple to complex adaptions, falls risk assessments in care environments and social settings, and targeted patient information/ media campaigns through to fracture liaison services.
Reflections
It remains important to focus on tertiary prevention and ensure the building blocks for health and wellbeing remain throughout the life-course. Digital and social connections to support prevention and treatment need to be available and suitable to provide equity in access, experience and outcomes. The prevention approach must be integrated and should support the individual rather than a specific care pathway, as there is much overlap in risk factors for falls and other related areas including frailty, dementia, bone health and multimorbidity. Tertiary prevention needs to support individuals to live their lives well and be empowered and supported to have the right social connections and opportunities, a warm and safe home and adequate healthy food.
Recommendations:
- There should be equity in access to services and all levels of preventative support including screening and vaccination, with proactive community engagement and reasonable adjustments where needed building on learning from outreach work during the pandemic.
7. Joint Strategic Needs Assessment (JSNA)
The Joint Strategic Needs Assessment (JSNA) in Devon looks to examine current and future health and wellbeing needs of the local population.
Devon is the third largest county in the country with beautiful natural environment and history attracting many residents and tourists to live and visit the area. Devon has great potential in providing individuals and families with the opportunity to live a healthy and fulfilled life. Like many areas, there are challenges which exist for Devon residents which can impact upon this ability to live a healthy life.
Devon has an ageing and growing population, with proportionately more older people compared to the England average. The total population for Devon is currently 814,440. The growth of Devon population is influenced by longer life expectancy, internal migration and increases in new developments across the county.
Figure 7.1: Census Population 2021, Devon
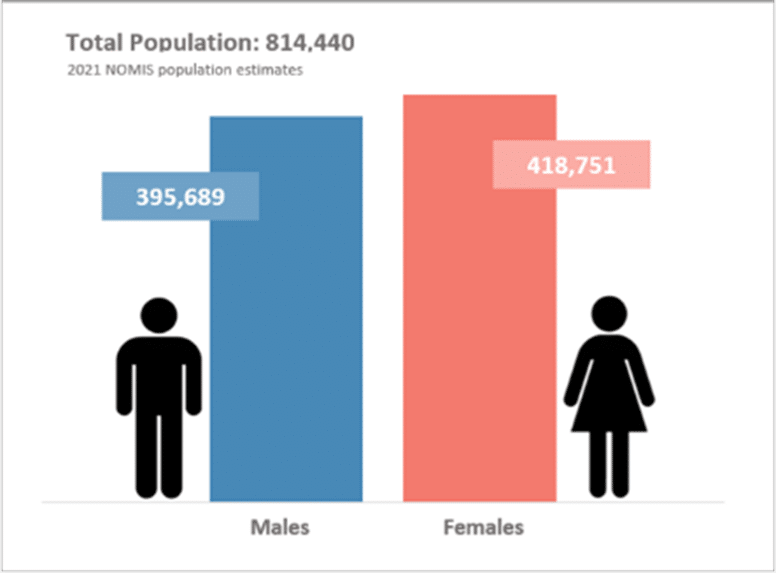
Source: NOMIS, 2023 Nomis – Official Census and Labour Market Statistics – Nomis – Official Census and Labour Market Statistics (nomisweb.co.uk)
Figure 7.2: Population Projections, Devon
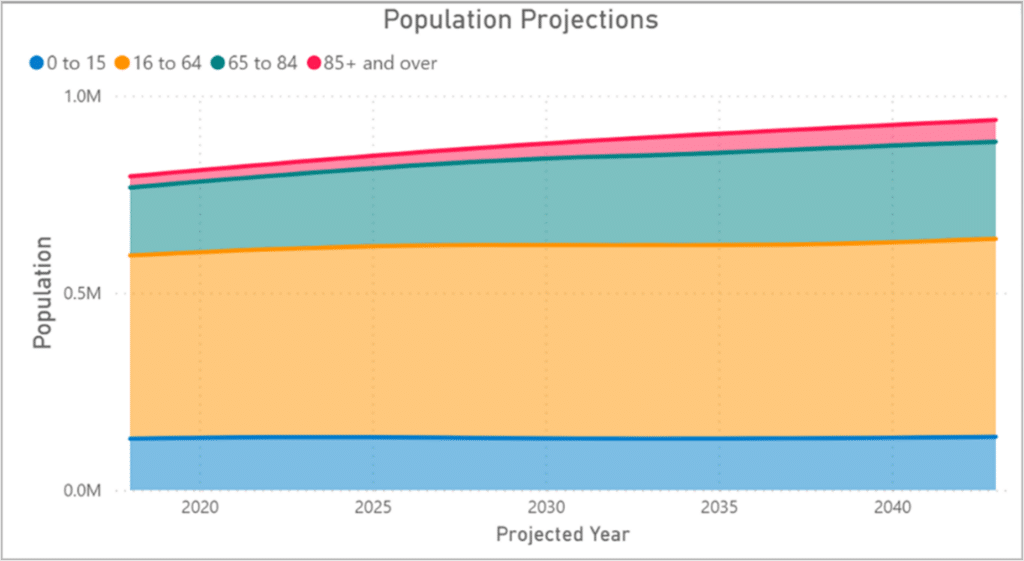
Source: NOMIS, 2023 Nomis – Official Census and Labour Market Statistics – Nomis – Official Census and Labour Market Statistics (nomisweb.co.uk)
Health and wellbeing outcomes are influenced by the conditions in society – where people are born, grow, live, work and age. Differences in health and wellbeing outcomes arise because of differences in society. These differences are referred to as inequalities in health and wellbeing. While across England we do not observe the extreme inequalities seen globally, inequality is still substantial and tackling these factors remains a priority.
Across Devon, people living in the poorer neighbourhoods tend to, on average, die between 5 and 7 years earlier that people living in more affluent neighbourhoods. However, the difference in life expectancy is even more stark in smaller areas such as Central Ilfracombe and Liverton in Exmouth where there is a staggering 15-year difference. Moreover, people in poorer areas also spend more of their shorter lives with a disability and/or in poorer heath.
Figure 7.3: Life and Healthy Life Expectancy, at birth
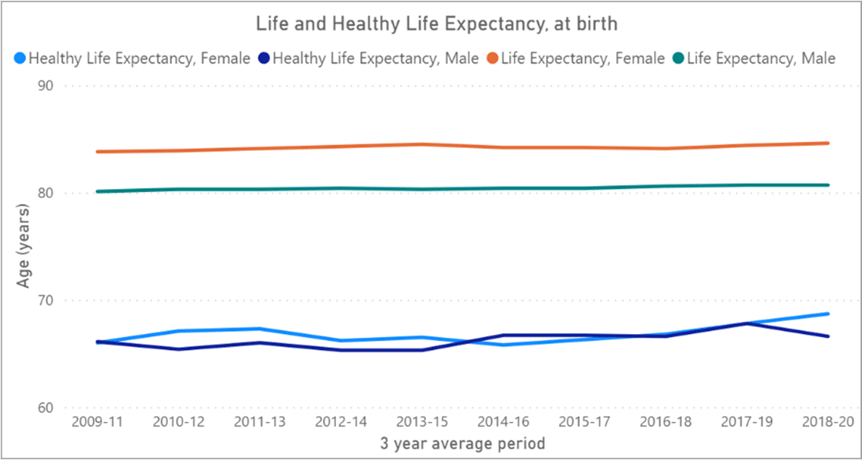
Source: ONS, 2023 Health and life expectancies – Office for National Statistics (ons.gov.uk)
Climate change is also already impacting health in a variety of ways, including leading to death and illness through increasing frequent extreme weather evens such as heatwaves, storms, floods, disruption to food systems, increases in communicable diseases, and mental health issues. Climate change risks undermining many of the social determinants for good health and wellbeing such as clean air, safe drinking water, sufficient food, and secure shelter.
Starting Well and Developing Well
Although there are proportionately fewer younger people in Devon compared nationally, there are considerable opportunities and benefits in ensuring children have the best start in life. It is well evidenced that what happens in early years, starting in the womb, has lifelong effects on a person’s health, wellbeing, and life chances.
Outcomes for children and young people across Devon are mixed. Across Devon there are considerable primary and secondary preventive opportunities in improving smoking during pregnancy, new birth visits and reviews, sustaining and improving breastfeeding, improving health protection measures such as handwashing and increasing immunisation coverage particularly for children in care.
A focus on improving behavioural risk factors for children and young people around diet and physical activity is required to reduce dental decay in younger children and obesity in primary and secondary school aged children.
Whilst a fair proportion of children at the end of reception reach a good level of development, around a quarter of pupils are not achieving this level which may have an impact throughout their life. This gap in school readiness is considerably wider for disadvantaged children.
Poor mental health in children results in poorer outcomes relating to health and wellbeing. Hospital admissions in children and young people are considerably higher in Devon for mental health conditions, self-harm, and injuries. This gap is even wider for vulnerable groups such as disadvantaged and looked after children.
Living and Working Well
Devon has proportionately fewer working age people compared to the England average, particularly in persons aged 16 to 49 years. Whilst the population of Devon continue to grow, the working age population is declining as a share. It is estimated that by 2031, the proportion of over 65s is expected to increase in Devon to almost 30%. Nationally, the proportion of over 65s is not expected to reach 25% until 2048.
The level of educational qualifications is similar in Devon compared with the national average; however, there are lower levels across certain areas within Devon. It is well evidence that educational qualifications are also a determinant of a person’s labour market position, which in turn influences income, housing and other material resources associated with health.
There is significant variation between areas within Devon in relation to economic landscape. Average earnings for Devon have been increasing at a slightly quicker rate compared to the UK, however average earnings overall in Devon are well below the national average. Across the districts in Devon, earnings are even lower with some of the lowest earnings observed in Torridge and North Devon.
Housing across Devon is expensive, making it a challenge for some lower income households to get on the property ladder. Those who live in rural communities are impacted even more by low wages, lack of access to affordable housing, public transport, and digital connectivity.
Behavioural risk factors such as Smoking, alcohol, poor diet and lack of physical activity are the leading influences of ill health and premature mortality both nationally and locally. The impact is even greater for those living in poorer neighbourhoods. Obesity continues to increase worldwide and the associated factors which influence obesity include deprivation, socioeconomic issues, poor diet and lack of physical activity have also been impacted by the COVID-19 pandemic and the cost-of-living crisis.
Poorer health can further manifest downstream. It can impact on the ability to work which may lead to receipt of state benefits and/or creating more cost across the health and social care system for treatment and support-based services. If the population of Devon are living between 10 to 15 years in poorer health and require treatment and support, evidently it will be significant and increasing cost to the system.
There are opportunities to improve primary and secondary prevention such as increasing immunisation and screening coverage and improving health protection measures to prevent ill health, reduce disease progression and mortality from many diseases.
Ageing and Dying Well
Devon has an ageing and growing population with proportionately more older people compared to England.
On average, life expectancy at 65 years for male and females in Devon is 20 and 22 years. Just under half of those years are spent in poorer health. This will have a significant impact on service cost and demand across the system particularly when considering the expected growth in our population over the coming 10 years.
Whilst Devon is generally less deprived overall relative to Devon, a third of the county is classified as rural which can present challenges around access to services and isolation contributing to poorer health.
The development of frailty, long term conditions and multi-morbidity is impacted greatly by social and behavioural risk factors. This can be influenced by poorer mental health or poor physical health may lead to poor mental health. This impact is even greater where inequalities are a considerable challenge.
Cancer, diseases of circulatory, respiratory, nervous system, and mental health and behavioural disorders are the leading causes of death across Devon. From a seasonal perspective, higher excess winter deaths occur in older people with pre – existing circulatory and respiratory diseases. Across Devon excess winter deaths have remained relatively unchanged. However increased uptake of primary and secondary interventions such as immunisations and screening programmes may help to reduce excess winter deaths.
Cancer screening for bowel has continued to increase, however cervical and breast screening across Devon is decreasing in woman aged 50 years and over. Early detection of cancer can improve cancer outcomes by providing care and treatment at the earliest possible stage. Reduced screening uptake may increase the risk of poorer cancer outcomes and preventable mortality.
Vaccination coverage for those aged 65 years and over, and at-risk individuals has improved since 2020 (85.3% and 60.3% respectively), a similar pattern nationally. Increases in vaccination coverage can be attributed to the proactive targeted work around COVID and Flu vaccination programme. However, continued work around increasing uptake in all groups remain a priority.
Dementia diagnosis remains unchanged in Devon and highlights a potential gap of unmet need where more than 2 in 5 people aged 65 and over are estimated to have dementia but are undiagnosed.
From an inequalities perspective immunisations and screening, and incidence and mortality rates may also differ when looking at more deprived areas and cohorts with protective characteristics. Therefore, in some instances the gap in outcomes may be wider.
To conclude, the Devon population is diverse in its needs and inequality can take many forms which impacts population health, to which organisations from across the system need to respond. As mentioned in the earlier part of this Annual Report, it is imperative that we as a system increase our focus and funding on prevention if we are to turn the tide on the stalling of life expectancy, improve health outcomes, address health inequalities, and critically help reduce demand on our heath and care system.
8. Update on recommendations from 2021-22

| Recommendations 2021-22 | Update on Progress |
| Public Health Devon continues to maintain a surveillance system to monitor local cases and outbreaks across settings to enable swift public health actions, working closely with our partners. | The Coronavirus dashboard was maintained and continued to inform action and monitor this phase of the pandemic response, it was helpful to monitor hospital related stays to understand pressure on the local system. As part of the living with covid plan and reduction in testing the data has become less reliable and the dashboard is no longer available with reliance on national sources |
| Public Health Devon continues to support NHS partners in the promotion and delivery of the COVID-19 vaccination programme, with a particular focus on addressing inequalities in uptake. | The award-winning vaccination health inequalities programme has maintained a focus on increasing uptake with continuation of a targeted outreach programme supported by engagement, communications and marketing and sharing of learning. |
| Further research should be commissioned to gain a greater understanding of food insecurity and fuel poverty in Devon, its impact and the arrangements to support people at greatest risk. | Both quantitative and qualitative research was commissioned by Public Health Devon. The findings of the food and fuel insecurity survey were widely disseminated. It showed that the number of households unable to access or afford the food they need to stay healthy had increased by 70% in 18 months and that more than a third of people were planning to switch off their heating altogether to help ends meet. Qualitative research has focused on the lived experience of people from Black, Asian and minority ethnic groups and families with multiple challenges, as well as the different food support options that are available in the county. |
| Increase in publicity to raise awareness and encourage eligible homeowners in Devon to access free energy efficiency improvements through Cosy Devon. | Energy Saving Devon (formerly Cosy Devon) has been promoting the support available for energy efficiency improvements to homes: our Local Community Energy Group – Energy Saving Devon. Cost of Living web pages and pop-up events throughout Devon have also been promoting availability of support. Fuel poverty pilots, run through Local Care Partnerships, have worked to help people at particular risk of poor health related to cold and damp (people with COPD and CVD for instance) to access energy efficiency improvements and wider signposting and support. |
| Public Health Devon works with NHS partners to ensure the learning from the delivery of the COVID-19 vaccination programme is embedded in the delivery of all routine vaccination programmes. | The NHS Integrated Care System Strategy and Joint Forward Plan have a health protection priority with a focus on inequalities in screening and immunisation programmes and the learning has and will continue to be shared |
| The Council continues to work with Government and local partners in the commissioning and delivery of schemes which mitigate some of the impacts of food and fuel insecurity, through funding within the Household Support Fund and Holiday Activities and Food programme. | The findings of all recent research, including the research commissioned by Public Health, is providing insight to guide the work of: 1 The Food Insecurity Sub-group which is linked to the VCSE Assembly and the Devon Strategic Food Partnership and 2: Energy Saving Devon (formerly the Cosy Devon Partnership). These partnerships can help identify the commissioning and delivery priorities for funding, for instance through the Household Support Fund and the Holiday Activity and Food programme. |
| Public Health Devon work collaboratively with colleagues from Education and children and young people service providers to explore the delivery of an enhanced health and wellbeing programme offer. | In collaboration with partners, Public Health Devon have established the Devon Schools Wellbeing Partnership, a free universal health and wellbeing programme for schools across Devon, to support schools to create environments that enable the wellbeing of pupils, staff, and wider school community.
Public Health Devon are also working with colleagues across local authority and health to embed a compassionate whole systems approach to healthier weight |
9. Acknowledgements and Further Information
If you would like this report in a different format, such as large print or Braille, please contact:
Public Health Devon, County Hall, Topsham Road, Exeter, EX2 4QD
Phone: 01392 383000
Email: publichealth@devon.gov.uk
This annual report has been written by Steven Brown with input from Lucy O’Loughlin, Maria Moloney-Lucey, Sara Gibbs, Simon Chant and Tina Henry.
Published by Devon County Council 2023
Copyright Devon County Council 2023